THE EFFECTS OF HEAD TRAUMA: INCREASED INTRACRANIAL PRESSURE
Neurological dysfunction and death in TBI are due to a) the brain injury itself, b) prolonged coma with its complications, c) infections from open wounds or basilar skull fractures, d) hydrocephalus from subarachnoid hemorrhage, and, most important, e) increased intracranial pressure. Increased intracranial pressure is caused by a) the added mass of epidural, subdural, and intracranial hematomas and b) cerebral edema that develops around large contusions, from diffuse vascular injury, and as a result of HIE. In infants, the skull can expand to some extent. After the sutures close, it is rigid. The brain and CSF are not compressible. Any increase in intracranial mass will first displace CSF into the spinal subarachnoid space. An increase of intracranial pressure above 40-50 mm Hg collapses brain capillaries, resulting in global ischemia.
HERNIATIONS
The cranial cavity is partitioned by the tentorium cerebelli and the falx cerebri. When a part of the brain is compressed by an extrinsic lesion such as a subdural hematoma or is expanded because of a brain tumor, abscess, or another intrinsic lesion, it is displaced (herniates) from one cranial compartment to another. Three major herniations can occur, either alone or in combination: Subfalcial herniation, uncal (transtentorial) herniation, and cerebellar tonsillar herniation.
 Subfalcial herniation |
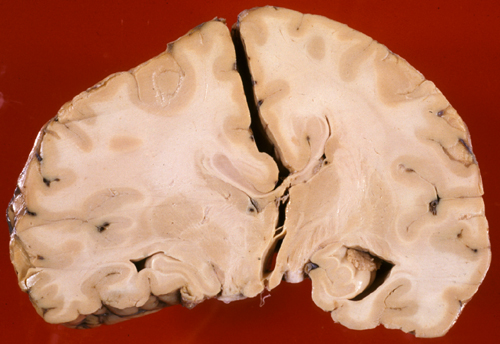
Subfalcial herniation is displacement of the cingulate gyrus from one hemisphere to the other, under the falx cerebri. Subfalcial herniation can compress the pericallosal arteries, causing an infarct in their distribution.
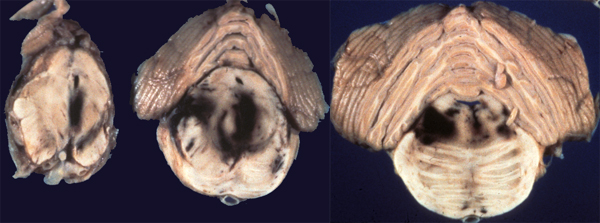 Secondary brainstem hemorrhages |
|
 Uncal herniation |
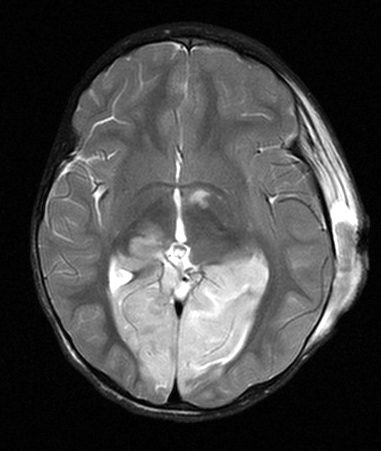 Bilateral PCA infarcts from uncal herniation |
Uncal (transtentorial) herniation is herniation of the medial temporal lobe from the middle into the posterior fossa, across the tentorial opening. The uncus of the temporal lobe is forced into the gap between the midbrain and the edge of the tentorium. This compresses the ipsilateral oculomotor nerve, causing a fixed and dilated pupil, and collapses the ipsilateral posterior cerebral artery, causing an infarct in its distribution. Cortical blindness resulting from this infarct is a false localizing sign because it gives the erroneous impression that the primary lesion is in the occipital lobe. As the herniating uncus displaces the midbrain laterally, the contralateral cerebral peduncle is compressed against the edge of the tentorium, causing paralysis on the same side as the primary lesion, another false localizing sign. Caudal displacement of the brainstem and stretching of its vessels causes a variety of hemorrhagic lesions in the midbrain and pons (secondary brainstem hemorrhages) that can devastate the reticular activating substance and other brainstem centers, resulting in focal neurological deficits and coma.
 Cerebellar tonsillar herniation |
Pressure on the posterior fossa contents from above or from within compresses the pons against the clivus and displaces the cerebellar tonsils into the foramen magnum (cerebellar tonsillar herniation). This may cause stiffness of the neck and head tilt. Compression of the pons and medulla damages vital centers for respiration and cardiac function, resulting in cardiorespiratory arrest.
CEREBRAL EDEMA
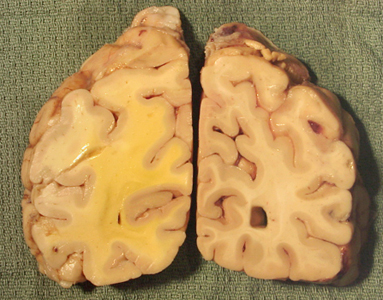 Edema around an adjacent hemorrhagic tumor |
 Papilledema |
 Normal white matter |
 Edematous white matter |
Cerebral edema in TBI, HIE, brain tumors, meningitis, brain abscess, and other pathologies is caused by accumulation of water in interstitial CNS spaces due to increased vascular permeability (vasogenic edema) and in some cases also by accumulation of water in injured cells (cytotoxic edema). Vasogenic edema involves more severely the white matter and extends along the optic nerves and into the optic papillae (papilledema). The edematous optic papillae protrude forward into the vitreous chamber and displace the retina, causing blurring of vision. Fundoscopic examination reveals blurred disk margins.
Understanding the anatomy and warning signs of herniations and promptly taking measures to reduce intracranial pressure will save lives. Herniations are important not only in trauma but in any condition associated with cerebral edema and increased intracranial pressure, including HIE, stroke, meningitis, brain abscess, brain tumors, and hydrocephalus.