Incorrect. Rheumatoid arthritis can cause interstitial inflammation, type 2 atrophy (due to immobilization) and, in advanced stages, a necrotizing vasculitis indistinguishable from polyarteritis nodosa.
Incorrect. Rheumatoid arthritis can cause interstitial inflammation, type 2 atrophy (due to immobilization) and, in advanced stages, a necrotizing vasculitis indistinguishable from polyarteritis nodosa.
Incorrect. Rheumatoid arthritis can cause interstitial inflammation, type 2 atrophy (due to immobilization) and, in advanced stages, a necrotizing vasculitis indistinguishable from polyarteritis nodosa.
Correct. Rheumatoid arthritis can cause interstitial inflammation, type 2 atrophy (due to immobilization) and, in advanced stages, a necrotizing vasculitis indistinguishable from polyarteritis nodosa.
Question 2: In denervation, the atrophic fibers are predominantly:
Incorrect. In denervation, both fiber types are affected. Denervation results in random atrophy of both type 1 and type 2 fibers, followed by fiber type grouping during reinnervation.
Incorrect. In denervation, both fiber types are affected. Denervation results in random atrophy of both type 1 and type 2 fibers, followed by fiber type grouping during reinnervation.
Correct. In denervation, both fiber types are affected. Denervation results in random atrophy of both type 1 and type 2 fibers, followed by fiber type grouping during reinnervation.
Question 3: A 61 year-old man developed hoarseness and subsequently weakness of the grip of one hand, then the other. Weakness progressed over 3 months. Sensation is normal and CK is normal. A quadriceps muscle biopsy is shown. The most likely cause of the illness is:
Incorrect. The picture shows myofiber atrophy, including group atrophy, consistent with denervation. The history suggests ALS, which is a sporadic neurodegenerative disease. CTG trinucleotide expansion is seen in myotonic dystrophy.
Correct. The picture shows myofiber atrophy, including group atrophy, consistent with denervation. The history suggests ALS, which is a sporadic neurodegenerative disease. CTG trinucleotide expansion is seen in myotonic dystrophy.
Incorrect. The picture shows myofiber atrophy, including group atrophy, consistent with denervation. The history suggests ALS, which is a sporadic neurodegenerative disease. CTG trinucleotide expansion is seen in myotonic dystrophy.
Incorrect. The picture shows myofiber atrophy, including group atrophy, consistent with denervation. The history suggests ALS, which is a sporadic neurodegenerative disease. CTG trinucleotide expansion is seen in myotonic dystrophy.
Question 4: CK of 4500 is most likely seen in:
Incorrect. A CK of 4,500 is most likely seen in the 27 year-old male with severe proximal weakness and a positive family history. This scenario suggests a dystrophinopathy, specifically Becker muscular dystrophy. The three-month-old hypotonic infant with fasciculations probably has spinal muscular atrophy. The 46-year-old woman with arthritis, etc probably has rheumatoid arthritis with superimposed polyarteritis nodosa.
Incorrect. A CK of 4,500 is most likely seen in the 27 year-old male with severe proximal weakness and a positive family history. This scenario suggests a dystrophinopathy, specifically Becker muscular dystrophy. The three-month-old hypotonic infant with fasciculations probably has spinal muscular atrophy. The 46-year-old woman with arthritis, etc probably has rheumatoid arthritis with superimposed polyarteritis nodosa.
Correct. A CK of 4,500 is most likely seen in the 27 year-old male with severe proximal weakness and a positive family history. This scenario suggests a dystrophinopathy, specifically Becker muscular dystrophy. The three-month-old hypotonic infant with fasciculations probably has spinal muscular atrophy. The 46-year-old woman with arthritis, etc probably has rheumatoid arthritis with superimposed polyarteritis nodosa.
Incorrect. A CK of 4,500 is most likely seen in the 27 year-old male with severe proximal weakness and a positive family history. This scenario suggests a dystrophinopathy, specifically Becker muscular dystrophy. The three-month-old hypotonic infant with fasciculations probably has spinal muscular atrophy. The 46-year-old woman with arthritis, etc probably has rheumatoid arthritis with superimposed polyarteritis nodosa.
Question 5: The most common cause of neuropathy in adults over 50 years is:
Incorrect. Diabetes mellitus is the most common cause of neuropathy in adults over 50 years of age.
Correct. Diabetes mellitus is the most common cause of neuropathy in adults over 50 years of age.
Incorrect. Diabetes mellitus is the most common cause of neuropathy in adults over 50 years of age.
Incorrect. Diabetes mellitus is the most common cause of neuropathy in adults over 50 years of age.
Question 6: Patients with congenital muscular dystrophy may also have:
Incorrect. Patients with certain forms of congenital muscular dystrophy caused by glycosylation defects (Walker-Warburg Syndrome, Fukuyama congenital muscular dystrophy, and muscle-eye-brain disease) may have eye abnormalities.
Correct. Patients with certain forms of congenital muscular dystrophy caused by glycosylation defects (Walker-Warburg Syndrome, Fukuyama congenital muscular dystrophy, and muscle-eye-brain disease) may have eye abnormalities.
Incorrect. Patients with certain forms of congenital muscular dystrophy caused by glycosylation defects (Walker-Warburg Syndrome, Fukuyama congenital muscular dystrophy, and muscle-eye-brain disease) may have eye abnormalities.
Incorrect. Patients with certain forms of congenital muscular dystrophy caused by glycosylation defects (Walker-Warburg Syndrome, Fukuyama congenital muscular dystrophy, and muscle-eye-brain disease) may have eye abnormalities.
Question 7: Severe hypotonia in the neonatal period is caused by a mutation or abnormality involving all of the following except:
Incorrect. Sarcoglycan mutations cause limb-girdle syndromes, including a severe childhood onset limb-girdle dystrophy, which mimics Duchenne muscular dystrophy but does not cause neonatal hypotonia. Merosin abnormality causes congenital muscular dystrophy. Alpha-actinin abnormalities cause nemaline myopathy. SMN mutations cause spinal muscular atrophy. The latter three entities cause neonatal hypotonia.
Correct. Sarcoglycan mutations cause limb-girdle syndromes, including a severe childhood onset limb-girdle dystrophy, which mimics Duchenne muscular dystrophy but does not cause neonatal hypotonia. Merosin abnormality causes congenital muscular dystrophy. Alpha-actinin abnormalities cause nemaline myopathy. SMN mutations cause spinal muscular atrophy. The latter three entities cause neonatal hypotonia.
Incorrect. Sarcoglycan mutations cause limb-girdle syndromes, including a severe childhood onset limb-girdle dystrophy, which mimics Duchenne muscular dystrophy but does not cause neonatal hypotonia. Merosin abnormality causes congenital muscular dystrophy. Alpha-actinin abnormalities cause nemaline myopathy. SMN mutations cause spinal muscular atrophy. The latter three entities cause neonatal hypotonia.
Incorrect. Sarcoglycan mutations cause limb-girdle syndromes, including a severe childhood onset limb-girdle dystrophy, which mimics Duchenne muscular dystrophy but does not cause neonatal hypotonia. Merosin abnormality causes congenital muscular dystrophy. Alpha-actinin abnormalities cause nemaline myopathy. SMN mutations cause spinal muscular atrophy. The latter three entities cause neonatal hypotonia.
Question 8: Severe hypotonia in the neonatal period can be caused by:
Incorrect. Neonatal hypotonia can be caused by all: severe neuronal migration defects, motor neuron disease such as SMA, and perinatal asphyxia.
Incorrect. Neonatal hypotonia can be caused by all: severe neuronal migration defects, motor neuron disease such as SMA, and perinatal asphyxia.
Incorrect. Neonatal hypotonia can be caused by all: severe neuronal migration defects, motor neuron disease such as SMA, and perinatal asphyxia.
Correct. Neonatal hypotonia can be caused by all: severe neuronal migration defects, motor neuron disease such as SMA, and perinatal asphyxia.
Question 9: A 3 year-old boy with weakness, seizures, and psychomotor retardation had the muscle biopsy shown below. Abnormal laboratory findings are less likely to include:
Incorrect. The picture shows ragged red fibers, indicating a mitochondrial myopathy. Mitochondrial abnormalities are associated with elevated serum lactate, elevated ammonia, and elevated alanine. Abnormal liver function tests would be less likely, although some mitochondrial depletion syndromes, e.g., Alpers-Hutenlocher syndrome, and other mitochondrial disorders may cause hepatopathy.
Correct. The picture shows ragged red fibers, indicating a mitochondrial myopathy. Mitochondrial abnormalities are associated with elevated serum lactate, elevated ammonia, and elevated alanine. Abnormal liver function tests would be less likely, although some mitochondrial depletion syndromes, e.g., Alpers-Hutenlocher syndrome, and other mitochondrial disorders may cause hepatopathy.
Incorrect. The picture shows ragged red fibers, indicating a mitochondrial myopathy. Mitochondrial abnormalities are associated with elevated serum lactate, elevated ammonia, and elevated alanine. Abnormal liver function tests would be less likely, although some mitochondrial depletion syndromes, e.g., Alpers-Hutenlocher syndrome, and other mitochondrial disorders may cause hepatopathy.
Incorrect. The picture shows ragged red fibers, indicating a mitochondrial myopathy. Mitochondrial abnormalities are associated with elevated serum lactate, elevated ammonia, and elevated alanine. Abnormal liver function tests would be less likely, although some mitochondrial depletion syndromes, e.g., Alpers-Hutenlocher syndrome, and other mitochondrial disorders may cause hepatopathy.
Question 10: The pathological changes in muscle shown below occur most frequently in patients with mitochondrial myopathies due to:
Correct. The electron micrograph shows mitochondrial abnormalities. Abnormal mitochondria and ragged red fibers are more common in mitochondrial DNA mutations.
Incorrect. The electron micrograph shows mitochondrial abnormalities. Abnormal mitochondria and ragged red fibers are more common in mitochondrial DNA mutations.
Incorrect. The electron micrograph shows mitochondrial abnormalities. Abnormal mitochondria and ragged red fibers are more common in mitochondrial DNA mutations.
Question 11: Which of the following is a trinucleotide repeat disorder?
Incorrect. Myotonic dystrophy is caused by a CTG trinucleotide repeat expansion.
Correct. Myotonic dystrophy is caused by a CTG trinucleotide repeat expansion.
Incorrect. Myotonic dystrophy is caused by a CTG trinucleotide repeat expansion.
Incorrect. Myotonic dystrophy is caused by a CTG trinucleotide repeat expansion.
Question 12: A 60 year-old woman has proximal weakness and a CK of 1800. The most likely cause is:
Incorrect. Among the listed conditions, the most likely cause of proximal weakness and elevated CK in a 60 year-old woman is polymyositis.
Incorrect. Among the listed conditions, the most likely cause of proximal weakness and elevated CK in a 60 year-old woman is polymyositis.
Correct. Among the listed conditions, the most likely cause of proximal weakness and elevated CK in a 60 year-old woman is polymyositis.
Incorrect. Among the listed conditions, the most likely cause of proximal weakness and elevated CK in a 60 year-old woman is polymyositis.
Question 13: Severe limb girdle muscle dystrophy may result from mutations of:
Incorrect. Severe childhood autosomal recessive muscular dystrophy is caused by mutations of gamma sarcoglycan. Dystrophinopathies also cause proximal weakness, similar to limb girdle dystrophies. However, the term limb girdle dystrophy refers to a group of disorders that are distinct from the dystrophinopathies.
Correct. Severe childhood autosomal recessive muscular dystrophy is caused by mutations of gamma sarcoglycan. Dystrophinopathies also cause proximal weakness, similar to limb girdle dystrophies. However, the term limb girdle dystrophy refers to a group of disorders that are distinct from the dystrophinopathies.
Incorrect. Severe childhood autosomal recessive muscular dystrophy is caused by mutations of gamma sarcoglycan. Dystrophinopathies also cause proximal weakness, similar to limb girdle dystrophies. However, the term limb girdle dystrophy refers to a group of disorders that are distinct from the dystrophinopathies.
Incorrect. Severe childhood autosomal recessive muscular dystrophy is caused by mutations of gamma sarcoglycan. Dystrophinopathies also cause proximal weakness, similar to limb girdle dystrophies. However, the term limb girdle dystrophy refers to a group of disorders that are distinct from the dystrophinopathies.
Question 14: Dystrophin is located:
Incorrect. Dystrophin is located inside the sarcolemma, just beneath the cell membrane, where it connects the cytoskeleton to the dystroglycan complex.
Incorrect. Dystrophin is located inside the sarcolemma, just beneath the cell membrane, where it connects the cytoskeleton to the dystroglycan complex.
Correct. Dystrophin is located inside the sarcolemma, just beneath the cell membrane, where it connects the cytoskeleton to the dystroglycan complex.
Incorrect. Dystrophin is located inside the sarcolemma, just beneath the cell membrane, where it connects the cytoskeleton to the dystroglycan complex.
Question 15: Which of the following is caused by T-cells attacking myofibers:
Incorrect. Polymyositis is caused by cytotoxic T-cells and macrophages, which invade and destroy myofibers.
Correct. Polymyositis is caused by cytotoxic T-cells and macrophages, which invade and destroy myofibers.
Incorrect. Polymyositis is caused by cytotoxic T-cells and macrophages, which invade and destroy myofibers.
Question 16: A baby boy who was severely hypotonic since birth died of respiratory insufficiency at 4 months of age. The muscle biopsy (ATPase stain) is shown below. The risk of subsequent siblings developing the same condition is:
Incorrect. The muscle biopsy shows fiber type grouping, consistent with denervation. The clinical and pathological diagnosis is spinal muscular atrophy. This is an autosomal recessive disorder. The risk to subsequent siblings is 25%.
Correct. The muscle biopsy shows fiber type grouping, consistent with denervation. The clinical and pathological diagnosis is spinal muscular atrophy. This is an autosomal recessive disorder. The risk to subsequent siblings is 25%.
Incorrect. The muscle biopsy shows fiber type grouping, consistent with denervation. The clinical and pathological diagnosis is spinal muscular atrophy. This is an autosomal recessive disorder. The risk to subsequent siblings is 25%.
Incorrect. The muscle biopsy shows fiber type grouping, consistent with denervation. The clinical and pathological diagnosis is spinal muscular atrophy. This is an autosomal recessive disorder. The risk to subsequent siblings is 25%.
Question 17: If a transected nerve is promptly and precisely reconnected:
Incorrect. Following transection, the distal stump degenerates and the neuronal body undergoes central chromatolysis. Then, the severed axon regenerates. Schwann cells distal to the transection proliferate and make new myelin. If the regenerating axon reconnects with its targets, the anatomy of the neuronal body is restored.
Correct. Following transection, the distal stump degenerates and the neuronal body undergoes central chromatolysis. Then, the severed axon regenerates. Schwann cells distal to the transection proliferate and make new myelin. If the regenerating axon reconnects with its targets, the anatomy of the neuronal body is restored.
Incorrect. Following transection, the distal stump degenerates and the neuronal body undergoes central chromatolysis. Then, the severed axon regenerates. Schwann cells distal to the transection proliferate and make new myelin. If the regenerating axon reconnects with its targets, the anatomy of the neuronal body is restored.
Incorrect. Following transection, the distal stump degenerates and the neuronal body undergoes central chromatolysis. Then, the severed axon regenerates. Schwann cells distal to the transection proliferate and make new myelin. If the regenerating axon reconnects with its targets, the anatomy of the neuronal body is restored.
Question 18: The illustrated pathology occurs in all of the following neuropathies except:
Incorrect. The picture shows hypertrophic neuropathy (concentric layers of Schwann cell processes and collagen around axons). Hypertrophic changes are not a feature of diabetic neuropathies but occur in the other 3 entities.
Correct. The picture shows hypertrophic neuropathy (concentric layers of Schwann cell processes and collagen around axons). Hypertrophic changes are not a feature of diabetic neuropathies but occur in the other 3 entities.
Incorrect. The picture shows hypertrophic neuropathy (concentric layers of Schwann cell processes and collagen around axons). Hypertrophic changes are not a feature of diabetic neuropathies but occur in the other 3 entities.
Incorrect. The picture shows hypertrophic neuropathy (concentric layers of Schwann cell processes and collagen around axons). Hypertrophic changes are not a feature of diabetic neuropathies but occur in the other 3 entities.
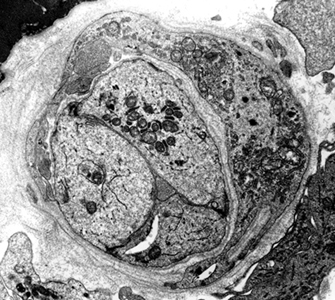
Question 19: The pathology illustrated in this nerve biopsy (low power EM) is caused by
Incorrect. The picture shows hypertrophic changes (concentric layers of Schwann cell processes and collagen). This pathology characterizes Charcot-Marie-Tooth type 1 neuropathy, which is due to duplication of a gene on chromosome 17p that encodes the protein PMP22.
Incorrect. The picture shows hypertrophic changes (concentric layers of Schwann cell processes and collagen). This pathology characterizes Charcot-Marie-Tooth type 1 neuropathy, which is due to duplication of a gene on chromosome 17p that encodes the protein PMP22.
Correct. The picture shows hypertrophic changes (concentric layers of Schwann cell processes and collagen). This pathology characterizes Charcot-Marie-Tooth type 1 neuropathy, which is due to duplication of a gene on chromosome 17p that encodes the protein PMP22.
Incorrect. The picture shows hypertrophic changes (concentric layers of Schwann cell processes and collagen). This pathology characterizes Charcot-Marie-Tooth type 1 neuropathy, which is due to duplication of a gene on chromosome 17p that encodes the protein PMP22.
Question 20: The highest CSF protein is seen in:
Correct. The highest CSF protein levels are seen in Guillain-Barré Syndrome, often with little or no pleocytosis (albuminocytologic dissociation).
Incorrect. The highest CSF protein levels are seen in Guillain-Barré Syndrome, often with little or no pleocytosis (albuminocytologic dissociation).
Incorrect. The highest CSF protein levels are seen in Guillain-Barré Syndrome, often with little or no pleocytosis (albuminocytologic dissociation).
Incorrect. The highest CSF protein levels are seen in Guillain-Barré Syndrome, often with little or no pleocytosis (albuminocytologic dissociation).
Question 21: Which of the following shows beta amyloid and tau deposits in muscle?
Incorrect. Inclusion body myositis is characterized by beta amyloid and tau protein deposits in muscle fibers, similar to those seen in Alzheimer's disease.
Incorrect. Inclusion body myositis is characterized by beta amyloid and tau protein deposits in muscle fibers, similar to those seen in Alzheimer's disease.
Correct. Inclusion body myositis is characterized by beta amyloid and tau protein deposits in muscle fibers, similar to those seen in Alzheimer's disease.
Incorrect. Inclusion body myositis is characterized by beta amyloid and tau protein deposits in muscle fibers, similar to those seen in Alzheimer's disease.
Question 22: The pathology in this muscle biopsy is from:
Incorrect. The pictures show muscle with perifascicular atrophy and a capillary with endothelial swelling, characteristic of dermatomyositis. The clinical history of the 4 year-old boy with weakness, GI bleed, and elevated CK is most consistent with this diagnosis.
Correct. The pictures show muscle with perifascicular atrophy and a capillary with endothelial swelling, characteristic of dermatomyositis. The clinical history of the 4 year-old boy with weakness, GI bleed, and elevated CK is most consistent with this diagnosis.
Incorrect. The pictures show muscle with perifascicular atrophy and a capillary with endothelial swelling, characteristic of dermatomyositis. The clinical history of the 4 year-old boy with weakness, GI bleed, and elevated CK is most consistent with this diagnosis.
Incorrect. The pictures show muscle with perifascicular atrophy and a capillary with endothelial swelling, characteristic of dermatomyositis. The clinical history of the 4 year-old boy with weakness, GI bleed, and elevated CK is most consistent with this diagnosis.
Question 23: CTG expansion in a neonate is manifested by:
Correct. CTG expansion causes myotonic dystrophy. Infantile myotonic dystrophy is characterized primarily by hypotonia without brain abnormalities on MRI.
Incorrect. CTG expansion causes myotonic dystrophy. Infantile myotonic dystrophy is characterized primarily by hypotonia without brain abnormalities on MRI.
Incorrect. CTG expansion causes myotonic dystrophy. Infantile myotonic dystrophy is characterized primarily by hypotonia without brain abnormalities on MRI.
Incorrect. CTG expansion causes myotonic dystrophy. Infantile myotonic dystrophy is characterized primarily by hypotonia without brain abnormalities on MRI.
Question 24: The illustrated findings are most consistent with:
Correct. The picture shows atrophic myofibers and central nuclei, which are most consistent with myotonic dystrophy, an autosomal dominant disorder.
Incorrect. The picture shows atrophic myofibers and central nuclei, which are most consistent with myotonic dystrophy, an autosomal dominant disorder.
Incorrect. The picture shows atrophic myofibers and central nuclei, which are most consistent with myotonic dystrophy, an autosomal dominant disorder.
Incorrect. The picture shows atrophic myofibers and central nuclei, which are most consistent with myotonic dystrophy, an autosomal dominant disorder.
Question 25: The pathology illustrated below is caused by:
Incorrect. The pathology shows centronuclear myopathy, a congenital myopathy. Some cases of centronuclear myopathy are X-linked.
Correct. The pathology shows centronuclear myopathy, a congenital myopathy. Some cases of centronuclear myopathy are X-linked.
Incorrect. The pathology shows centronuclear myopathy, a congenital myopathy. Some cases of centronuclear myopathy are X-linked.
Incorrect. The pathology shows centronuclear myopathy, a congenital myopathy. Some cases of centronuclear myopathy are X-linked.