Incorrect. In a general community hospital setting, metastatic brain tumors are more common.
Correct. In a general community hospital setting, metastatic brain tumors are more common.
Question 2: A child with craniospinal irradiation for ALL has a higher risk for developing an astrocytoma compared to other children
Correct.
Incorrect.
Question 3: Radiation to the head and neck is a risk factor for subsequent development of meningioma
Correct. Radiation to the head and neck, even in small amounts, is a risk factor for the subsequent development of meningioma.
Incorrect. Radiation to the head and neck, even in small amounts, is a risk factor for the subsequent development of meningioma.
Question 4: Homer-Wright rosettes are relatively uncommon in medulloblastoma
Correct. Homer-Wright rosettes have a high diagnostic value but are seen in a minority of tumors. Most medulloblastomas show diffuse sheets of small blue cells without rosettes.
Incorrect. Homer-Wright rosettes have a high diagnostic value but are seen in a minority of tumors. Most medulloblastomas show diffuse sheets of small blue cells without rosettes.
Question 5: Most primary cerebral lymphomas are:
Incorrect.
Correct.
Incorrect.
Question 6: Low grade tumors have as many but different chromosomal abnormalities as high grade tumors do
Incorrect. The more malignant the tumor, the more numerous and complex the chromosomal and molecular changes.
Correct. The more malignant the tumor, the more numerous and complex the chromosomal and molecular changes.
Question 7: A 5 year old boy had multifocal brain lesions one of which is shown below. The most likely underlying factor is:
Correct. The large perivascular mononuclear cells suggest CNS lymphoma. This would be most compatible with genetic immunodeficiency.
Incorrect. The large perivascular mononuclear cells suggest CNS lymphoma. This would be most compatible with genetic immunodeficiency.
Incorrect. The large perivascular mononuclear cells suggest CNS lymphoma. This would be most compatible with genetic immunodeficiency.
Incorrect. The large perivascular mononuclear cells suggest CNS lymphoma. This would be most compatible with genetic immunodeficiency.
Question 8: Which of the following are the most ubiquitous neurocarcinogens?
Incorrect.
Incorrect.
Correct.
Incorrect.
Question 9: Which of the following is not a feature of pilocytic astrocytoma?
Incorrect.
Correct.
Incorrect.
Incorrect.
Incorrect.
Question 10: What finding distinguishes glioblastoma multiforme from lower grade astrocytomas?
Incorrect.
Incorrect.
Correct.
Incorrect.
Question 11: Which of the following lesions extends across the corpus callosum?
Incorrect.
Incorrect.
Incorrect.
Correct.
Question 12: Which of the following may present as a ring enhancing lesion?
Incorrect.
Incorrect.
Incorrect.
Correct.
Question 13: A 3 year old boy with a history of headaches and morning vomiting for 10 days presents to the ER after a bad episode of vomiting. He is afebrile. The diagnostic studies might include all of the following except:
Incorrect. The symptoms suggest increased intracranial pressure. A spinal tap is contraindicated.
Correct. The symptoms suggest increased intracranial pressure. A spinal tap is contraindicated.
Incorrect. The symptoms suggest increased intracranial pressure. A spinal tap is contraindicated.
Incorrect. The symptoms suggest increased intracranial pressure. A spinal tap is contraindicated.
Question 14: The most common intracranial site of germ cell tumors is:
Correct.
Incorrect.
Incorrect.
Incorrect.
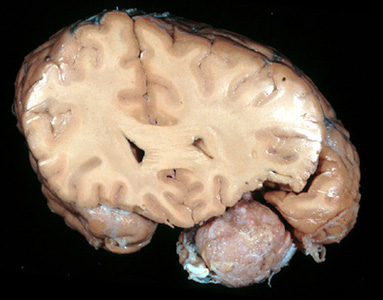
Question 15: Which of the following statements about the posterior fossa lesion shown below is not true?
Incorrect. The image shows a glioma composed of alternating dense fibrous areas and loose microcystic areas, consistent with a pilocytic astrocytoma. PAs do not evolve into malignant forms. Other astrocytomas do.
Correct. The image shows a glioma composed of alternating dense fibrous areas and loose microcystic areas, consistent with a pilocytic astrocytoma. PAs do not evolve into malignant forms. Other astrocytomas do.
Incorrect. The image shows a glioma composed of alternating dense fibrous areas and loose microcystic areas, consistent with a pilocytic astrocytoma. PAs do not evolve into malignant forms. Other astrocytomas do.
Incorrect. The image shows a glioma composed of alternating dense fibrous areas and loose microcystic areas, consistent with a pilocytic astrocytoma. PAs do not evolve into malignant forms. Other astrocytomas do.
Incorrect. The image shows a glioma composed of alternating dense fibrous areas and loose microcystic areas, consistent with a pilocytic astrocytoma. PAs do not evolve into malignant forms. Other astrocytomas do.
Question 16: Which of the following statements about the lesion illustrated below is not true?
Incorrect. The top image shows a hemorrhagic mass in the 4th ventricle protruding through the foramen of Lushka. The bottom image is a microscopic view of the tumor and shows tubular structures (true rosettes). The findings are consistent with an ependymoma. Although ependymomas bathe in CSF, they do not cause CSF seeding as frequently as medulloblastomas do.
Correct. The left image shows a hemorrhagic mass in the
4th ventricle protruding through the foramen of Lushka. The image on the right is a microscopic view of the tumor and shows tubular structures (true rosettes). The findings are consistent with an ependymoma. Although ependymomas bathe in CSF, they do not cause CSF seeding as frequently as medulloblastomas do.
Incorrect. The left image shows a hemorrhagic mass in the
4th ventricle protruding through the foramen of Lushka. The image on the right is a microscopic view of the tumor and shows tubular structures (true rosettes). The findings are consistent with an ependymoma. Although ependymomas bathe in CSF, they do not cause CSF seeding as frequently as medulloblastomas do.
Incorrect. The left image shows a hemorrhagic mass in the
4th ventricle protruding through the foramen of Lushka. The image on the right is a microscopic view of the tumor and shows tubular structures (true rosettes). The findings are consistent with an ependymoma. Although ependymomas bathe in CSF, they do not cause CSF seeding as frequently as medulloblastomas do.
Incorrect. The left image shows a hemorrhagic mass in the
4th ventricle protruding through the foramen of Lushka. The image on the right is a microscopic view of the tumor and shows tubular structures (true rosettes). The findings are consistent with an ependymoma. Although ependymomas bathe in CSF, they do not cause CSF seeding as frequently as medulloblastomas do.
Question 17: Which of the following statements about the brain tumor in a 3 year old boy shown below is not true?
Incorrect. The picture shows a diffuse small blue cell tumor. In a 3 year old patient, the main considerations are a medulloblastoma or a supratentorial PNET. Medulloblastoma, a tumor of the cerebellum, is more common. Most medulloblastomas present with signs of increased intracranial pressure rather than ataxia.
Incorrect. The picture shows a diffuse small blue cell tumor. In a 3 year old patient, the main considerations are a medulloblastoma or a supratentorial PNET. Medulloblastoma, a tumor of the cerebellum, is more common. Most medulloblastomas present with signs of increased intracranial pressure rather than ataxia.
Incorrect. The picture shows a diffuse small blue cell tumor. In a 3 year old patient, the main considerations are a medulloblastoma or a supratentorial PNET. Medulloblastoma, a tumor of the cerebellum, is more common. Most medulloblastomas present with signs of increased intracranial pressure rather than ataxia.
Incorrect. The picture shows a diffuse small blue cell tumor. In a 3 year old patient, the main considerations are a medulloblastoma or a supratentorial PNET. Medulloblastoma, a tumor of the cerebellum, is more common. Most medulloblastomas present with signs of increased intracranial pressure rather than ataxia.
Correct. The picture shows a diffuse small blue cell tumor. In a 3 year old patient, the main considerations are a medulloblastoma or a supratentorial PNET. Medulloblastoma, a tumor of the cerebellum, is more common. Most medulloblastomas present with signs of increased intracranial pressure rather than ataxia.
Question 18: A 4 year old boy with a history of headaches and on-and-off vomiting for 2 weeks had the MRI findings shown below. The most likely diagnosis is:
Correct. The T2 MRI shows enlargement of the ventricles and transependymal edema. The findings indicate acute hydrocephalus which, in this case, is caused by a posterior fossa tumor. The recent onset of symptoms of increased intracranial pressure is most consistent with a medulloblastoma. Although ependymoma of the 4th ventricle can block CSF flow, it causes hydrocephalus less frequently than medulloblastoma does, and the course is more protracted. Glioblastoma of the cerebellum is uncommon. Aqueductal stenosis would be of much longer duration.
Incorrect. The T2 MRI shows enlargement of the ventricles and transependymal edema. The findings indicate acute hydrocephalus which, in this case, is caused by a posterior fossa tumor. The recent onset of symptoms of increased intracranial pressure is most consistent with a medulloblastoma. Although ependymoma of the 4th ventricle can block CSF flow, it causes hydrocephalus less frequently than medulloblastoma does, and the course is more protracted. Glioblastoma of the cerebellum is uncommon. Aqueductal stenosis would be of much longer duration.
Incorrect. The T2 MRI shows enlargement of the ventricles and transependymal edema. The findings indicate acute hydrocephalus which, in this case, is caused by a posterior fossa tumor. The recent onset of symptoms of increased intracranial pressure is most consistent with a medulloblastoma. Although ependymoma of the 4th ventricle can block CSF flow, it causes hydrocephalus less frequently than medulloblastoma does, and the course is more protracted. Glioblastoma of the cerebellum is uncommon. Aqueductal stenosis would be of much longer duration.
Incorrect. The T2 MRI shows enlargement of the ventricles and transependymal edema. The findings indicate acute hydrocephalus which, in this case, is caused by a posterior fossa tumor. The recent onset of symptoms of increased intracranial pressure is most consistent with a medulloblastoma. Although ependymoma of the 4th ventricle can block CSF flow, it causes hydrocephalus less frequently than medulloblastoma does, and the course is more protracted. Glioblastoma of the cerebellum is uncommon. Aqueductal stenosis would be of much longer duration.
Question 19: Which of the following statements about the lesion shown below is not true?
Incorrect. The picture shows whorls of tumor cells and a psammoma body (meningioma). Most meningiomas are benign and do not invade the brain.
Incorrect. The picture shows whorls of tumor cells and a psammoma body (meningioma). Most meningiomas are benign and do not invade the brain.
Incorrect. The picture shows whorls of tumor cells and a psammoma body (meningioma). Most meningiomas are benign and do not invade the brain.
Correct. The picture shows whorls of tumor cells and a psammoma body (meningioma). Most meningiomas are benign and do not invade the brain.
Incorrect. The picture shows whorls of tumor cells and a psammoma body (meningioma). Most meningiomas are benign and do not invade the brain.
Question 20: Which of the statements about the lesion shown below is not true?
Incorrect. The image shows an extra-axial mass located, roughly, between the sphenoid ridge and the frontal lobe, consistent with a meningioma. Recurrence of meningioma is usually due to incomplete primary resection, not malignancy.
Correct. The image shows an extra-axial mass located, roughly, between the sphenoid ridge and the frontal lobe, consistent with a meningioma. Recurrence of meningioma is usually due to incomplete primary resection, not malignancy.
Incorrect. The image shows an extra-axial mass located, roughly, between the sphenoid ridge and the frontal lobe, consistent with a meningioma. Recurrence of meningioma is usually due to incomplete primary resection, not malignancy.
Incorrect. The image shows an extra-axial mass located, roughly, between the sphenoid ridge and the frontal lobe, consistent with a meningioma. Recurrence of meningioma is usually due to incomplete primary resection, not malignancy.
Question 21: Which of the following statements about the illustrated lesion is not true?
Incorrect. The picture shows a spindle cell tumor with a palisading pattern characteristic of schwannoma. It is a component of neurofibromatosis 2, not neurofibromatosis 1.
Correct. The picture shows a spindle cell tumor with a palisading pattern characteristic of schwannoma. It is a component of neurofibromatosis 2, not neurofibromatosis 1.
Incorrect. The picture shows a spindle cell tumor with a palisading pattern characteristic of schwannoma. It is a component of neurofibromatosis 2, not neurofibromatosis 1.
Incorrect. The picture shows a spindle cell tumor with a palisading pattern characteristic of schwannoma. It is a component of neurofibromatosis 2, not neurofibromatosis 1.
Incorrect. The picture shows a spindle cell tumor with a palisading pattern characteristic of schwannoma. It is a component of neurofibromatosis 2, not neurofibromatosis 1.
Question 22: Which of the following statements about the lesion shown below is not true?
Incorrect. The left image shows an irregularly enlarged and
tortuous nerve which is consistent with a plexiform neurofibroma. The right image is a microscopic view of the tumor and shows nerve fascicles that are expanded because of a proliferation of neoplastic cells. This lesion arises in peripheral nerves and spinal roots.
It does not arise in the optic nerve. Optic nerve glioma is also seen in neurofibromatosis 1.
Incorrect. The left image shows an irregularly enlarged and tortuous nerve
which is consistent with a plexiform neurofibroma. The right image is a microscopic view of the tumor and shows nerve fascicles that are expanded because of a proliferation of neoplastic cells. This lesion arises in peripheral nerves and spinal roots. It does not arise in the optic nerve. Optic nerve glioma is also seen in neurofibromatosis 1.
Correct. The left image shows an irregularly enlarged
and tortuous nerve which is consistent with a plexiform neurofibroma. The right om image is a microscopic view of the tumor and shows nerve fascicles that are expanded because of a proliferation of neoplastic cells. This lesion arises in peripheral nerves and spinal roots. It does not arise in the optic nerve. Optic nerve glioma is also seen in neurofibromatosis 1.
Incorrect. The leftmage shows an irregularly enlarged and
tortuous nerve which is consistent with a plexiform neurofibroma. The right image is a microscopic view of the tumor and shows nerve fascicles that are expanded because of a proliferation of neoplastic cells. This lesion arises in peripheral nerves and spinal roots. It does not arise in the optic nerve. Optic nerve glioma is also seen in neurofibromatosis 1.
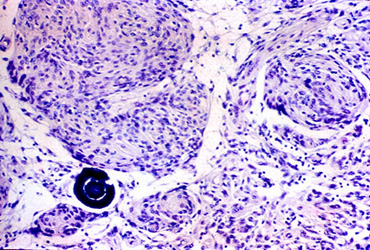
Question 23: Which of the following is not a feature of the illustrated lesion?
Correct. The image shows an epithelial tumor with loose microcystic areas and calcifications (the dark blue foci), consistent with a craniopharyngioma. Craniopharyngioma is a suprasellar tumor.
Incorrect. The image shows an epithelial tumor with loose microcystic areas and calcifications (the dark blue foci), consistent with a craniopharyngioma. Craniopharyngioma is a suprasellar tumor.
Incorrect. The image shows an epithelial tumor with loose microcystic areas and calcifications (the dark blue foci), consistent with a craniopharyngioma. Craniopharyngioma is a suprasellar tumor.
Incorrect. The image shows an epithelial tumor with loose microcystic areas and calcifications (the dark blue foci), consistent with a craniopharyngioma. Craniopharyngioma is a suprasellar tumor.
Incorrect. The image shows an epithelial tumor with loose microcystic areas and calcifications (the dark blue foci), consistent with a craniopharyngioma. Craniopharyngioma is a suprasellar tumor.
Question 24: A 43 year old HIV patient has had headaches and declining mental function for 5 weeks. MRI shows mild hydrocephalus with periventricular enhancing lesions. A stereotactic biopsy is obtained (shown below). The most likely diagnosis is:
Incorrect. The biopsy shows perivascular lymphoid cells with anaplasia, consistent with cerebral lymphoma.
Incorrect. The biopsy shows perivascular lymphoid cells with anaplasia, consistent with cerebral lymphoma.
Correct. The biopsy shows perivascular lymphoid cells with anaplasia, consistent with cerebral lymphoma.
Incorrect. The biopsy shows perivascular lymphoid cells with anaplasia, consistent with cerebral lymphoma.
Incorrect. The biopsy shows perivascular lymphoid cells with anaplasia, consistent with cerebral lymphoma.
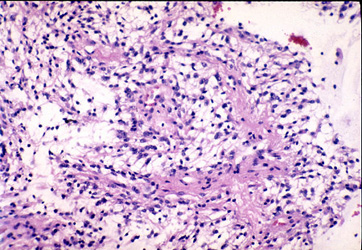
Question 25: A 42 year old woman had right-sided weakness progressing to hemiparesis in 3 to 4 weeks. MRI shows an enhancing lesion in the left centrum semiovale adjacent to the corpus callosum. A stereotactic biopsy is obtained (shown below). The findings suggest:
Correct. The image shows a poorly-defined inflammatory lesion with two areas of perivascular small lymphocytes. The pathology, together with rapid onset of the neurological deficit and the location of the lesion, is most consistent with an inflammatory demyelinative disease, acute MS or ADEM.
Incorrect. The image shows a poorly-defined inflammatory lesion with two areas of perivascular small lymphocytes. The pathology, together with rapid onset of the neurological deficit and the location of the lesion, is most consistent with an inflammatory demyelinative disease, acute MS or ADEM.
Incorrect. The image shows a poorly-defined inflammatory lesion with two areas of perivascular small lymphocytes. The pathology, together with rapid onset of the neurological deficit and the location of the lesion, is most consistent with an inflammatory demyelinative disease, acute MS or ADEM.
Incorrect. The image shows a poorly-defined inflammatory lesion with two areas of perivascular small lymphocytes. The pathology, together with rapid onset of the neurological deficit and the location of the lesion, is most consistent with an inflammatory demyelinative disease, acute MS or ADEM.
Incorrect. The image shows a poorly-defined inflammatory lesion with two areas of perivascular small lymphocytes. The pathology, together with rapid onset of the neurological deficit and the location of the lesion, is most consistent with an inflammatory demyelinative disease, acute MS or ADEM.
Question 26: A 57 year old patient had fever, seizures and obtundation for 4 days. MRI shows a necrotic hemorrhagic lesion of the right temporal lobe with surrounding edema. A stereotactic biopsy is shown below. The histology is most consistent with:
Incorrect. An acute inflammatory, hemorrhagic lesion in the temporal lobe is most consistent with HSV encephalitis.
Incorrect. An acute inflammatory, hemorrhagic lesion in the temporal lobe is most consistent with HSV encephalitis.
Incorrect. An acute inflammatory, hemorrhagic lesion in the temporal lobe is most consistent with HSV encephalitis.
Correct. An acute inflammatory, hemorrhagic lesion in the temporal lobe is most consistent with HSV encephalitis.
Question 27: A 6 year old girl with diabetes insipidus, visual disturbances, and headaches for 3 weeks had an MRI scan showing a 2 cm suprasellar mass and mild hydrocephalus. A stereotactic biopsy is shown below. The pathology is consistent with:
Incorrect. The histology of the lesion (islands of large clear cells with lymphocytic infiltrates) is consistent with a germ cell tumor (seminoma). The pineal and suprasellar regions are the most common sites of intracranial germ cell tumors.
Correct. The histology of the lesion (islands of large clear cells with lymphocytic infiltrates) is consistent with a germ cell tumor (seminoma). The pineal and suprasellar regions are the most common sites of intracranial germ cell tumors.
Incorrect. The histology of the lesion (islands of large clear cells with lymphocytic infiltrates) is consistent with a germ cell tumor (seminoma). The pineal and suprasellar regions are the most common sites of intracranial germ cell tumors.
Incorrect. The histology of the lesion (islands of large clear cells with lymphocytic infiltrates) is consistent with a germ cell tumor (seminoma). The pineal and suprasellar regions are the most common sites of intracranial germ cell tumors.
Question 28: A 27 year old woman with headaches and vomiting had a cystic cerebellar mass with a protruding nodule. Stereotactic biopsy is shown below. The pathology is consistent with:
Incorrect. The two images show aspects of a hemangioblastoma. The image on the right shows the vascularity of the tumor. The image on the left shows clear cells which are a component of the tumor.
Correct. The two images show aspects of a hemangioblastoma. The image on the right shows the vascularity of the tumor. The image on the left shows clear cells which are a component of the tumor.
Incorrect. The two images show aspects of a hemangioblastoma. The image on the right shows the vascularity of the tumor. The image on the left shows clear cells which are a component of the tumor.
Incorrect. The two images show aspects of a hemangioblastoma. The image on the right shows the vascularity of the tumor. The image on the left shows clear cells which are a component of the tumor.
Question 29: The illustrated structures may be present in:
Incorrect. The picture shows granular eosinophilic droplets. GEDs are seen in pilocytic astrocytoma and oligodendroglioma.
Incorrect. The picture shows granular eosinophilic droplets. GEDs are seen in pilocytic astrocytoma and oligodendroglioma.
Correct. The picture shows granular eosinophilic droplets. GEDs are seen in pilocytic astrocytoma and oligodendroglioma.
Incorrect. The picture shows granular eosinophilic droplets. GEDs are seen in pilocytic astrocytoma and oligodendroglioma.
Question 30: A previously healthy 53 year old man had an insidious onset of headaches, obtundation, and facial paralysis. CSF shows 33 lymphocytes, glucose 36, and protein 72. The most likely diagnosis is:
Correct. The clinical presentation and CSF profile are consistent either with meningeal carcinomatosis or with tuberculous meningitis. Tuberculous meningitis would be expected to have fever and symptoms of infection. Insidious presentation in a 50 year old healthy person is more consistent with carcinomatosis from an occult primary.
Incorrect. The clinical presentation and CSF profile are consistent either with meningeal carcinomatosis or with tuberculous meningitis. Tuberculous meningitis would be expected to have fever and symptoms of infection. Insidious presentation in a 50 year old healthy person is more consistent with carcinomatosis from an occult primary.
Incorrect. The clinical presentation and CSF profile are consistent either with meningeal carcinomatosis or with tuberculous meningitis. Tuberculous meningitis would be expected to have fever and symptoms of infection. Insidious presentation in a 50 year old healthy person is more consistent with carcinomatosis from an occult primary.
Incorrect. The clinical presentation and CSF profile are consistent either with meningeal carcinomatosis or with tuberculous meningitis. Tuberculous meningitis would be expected to have fever and symptoms of infection. Insidious presentation in a 50 year old healthy person is more consistent with carcinomatosis from an occult primary.
Question 31: The most common tumors of the pineal gland are:
Incorrect.
Correct.
Incorrect.
Question 32: You are called to the OR to do a frozen section of a suprasellar mass in a 5 year old boy. Which of the following would be most likely?
Incorrect. Pilocytic astrocytoma, followed by a craniopharyngioma, is the most common suprasellar tumor in children.
Correct. Pilocytic astrocytoma, followed by a craniopharyngioma, is the most common suprasellar tumor in children.
Incorrect. Pilocytic astrocytoma, followed by a craniopharyngioma, is the most common suprasellar tumor in children.
Incorrect. Pilocytic astrocytoma, followed by a craniopharyngioma, is the most common suprasellar tumor in children.
Question 33: A three year old boy had a cerebellopontine angle tumor with the ultrastructural features illustrated below.
Incorrect. The key EM findings are microvilli and dense junction, consistent with ependymoma.
Correct. The key EM findings are microvilli and dense junction, consistent with ependymoma.
Incorrect. The key EM findings are microvilli and dense junction, consistent with ependymoma.
Incorrect. The key EM findings are microvilli and dense junction, consistent with ependymoma.
Question 34: Which of the following statements about the lesion shown below is not true?
Incorrect. The illustrated lesion is a craniopharyngioma, not a benign teratoma. The image on the left shows an irregular epithelial island with microcystic change. This pattern is similar to ameloblastoma. The image on the right shows calcified masses of keratin. There are no mesodermal or endodermal derivatives. However, teratomas and other germ cell tumors also arise in a suprasellar location.
Incorrect. The illustrated lesion is a craniopharyngioma, not a benign teratoma. The image on the left shows an irregular epithelial island with microcystic change. This pattern is similar to ameloblastoma. The image on the right shows calcified masses of keratin. There are no mesodermal or endodermal derivatives. However, teratomas and other germ cell tumors also arise in a suprasellar location.
Correct. The illustrated lesion is a craniopharyngioma, not a benign teratoma. The image on the left shows an irregular epithelial island with microcystic change. This pattern is similar to ameloblastoma. The image on the right shows calcified masses of keratin. There are no mesodermal or endodermal derivatives. However, teratomas and other germ cell tumors also arise in a suprasellar location.
Incorrect. The illustrated lesion is a craniopharyngioma, not a benign teratoma. The image on the left shows an irregular epithelial island with microcystic change. This pattern is similar to ameloblastoma. The image on the right shows calcified masses of keratin. There are no mesodermal or endodermal derivatives. However, teratomas and other germ cell tumors also arise in a suprasellar location.